Bile duct cancer (also known as cholangiocarcinoma) is a rare malignant tumor that develops from cells internal lining of the bile ducts. The disease can be asymptomatic, and therefore the treatment of bile duct cancer often begins in the later stages. In addition, malignant tumors in this place are very "uncomfortable", and their surgical removal is difficult.
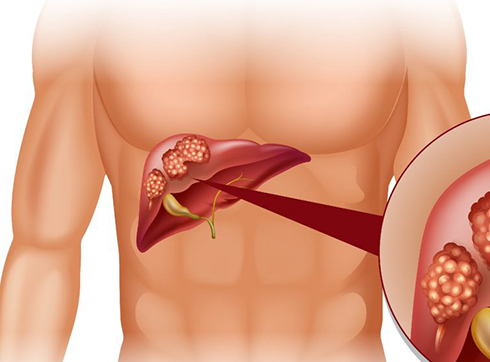
The liver is pierced by intrahepatic bile ducts, which unite at the exit from the liver into the common hepatic duct. The gallbladder is located under the liver. The bile duct comes out of it, which combines with the hepatic duct into the common bile duct (choledochus). The latter then unites with the pancreatic duct and opens into the duodenum. Tumors can develop anywhere in these intrahepatic and extrahepatic bile ducts.
Types of bile duct cancer
According to the histological structure of the tumor in the bile ducts, i.e. According to the type of cells in which it was formed, the following types of cancer are distinguished:
- Adenocarcinoma is a malignant neoplasm that develops from the glandular cells of the inner lining of the ducts - this is the most common cancer of the bile ducts;
- squamous cell carcinoma - from squamous epithelial cells;
- lymphoma - from cells of lymphoid tissue;
- sarcoma - from connective tissue cells.
A very common form of cancer of the liver or bile ducts is metastatic cancer, which has arisen from tumor cells (metastases) that have got here through the bloodstream or lymph from other organs. In this case, differential diagnosis is needed to determine the primary tumor and, accordingly, cancer treatment methods are selected, depending on its original nature. In our clinic, the root cause of bile duct cancer is precisely determined, which allows choosing the most effective treatment.
According to the localization of the tumor in the biliary tract, they are distinguished:
- Intrahepatic cholangiocarcinoma - this is slightly less common and can be confused with liver cancer (hepatocellular carcinoma).
- Extrahepatic cholangiocarcinoma, which is divided into the following types:
- Proximal, or hilus, cholangiocarcinoma - it is localized to the confluence of the bile and hepatic ducts, i.e. closer to the liver. This type of bile duct cancer is more common - in more than half of cases.
- Distal cholangiocarcinoma - it is located further from the liver and closer to the place where the common bile duct enters the duodenum. It is sometimes difficult to distinguish from pancreatic cancer.
In terms of surgical options for cancer treatment, neoplasms are divided into resectable tumors (they can be removed with a surgical operation) and unresectable (they are in hard-to-reach places or have spread greatly).
Causes of bile duct cancer
The root cause of any malignant neoplasms is mutations in normal cells that cause these cells to divide uncontrollably. But the causes of these mutations are not fully understood. However, there are risk factors that contribute to a higher likelihood of mutations and tumor development in the bile ducts.
Such risk factors include:
- Male gender. Bile duct cancer is more common in men.
- Age. With age, the number of mutations in cells accumulates, so the likelihood of carcinogenic mutations increases.
- Inflammation. The inflammatory process increases the risk of cancer cells. In the case of the bile ducts, the primary sclerosing cholangitis disease is dangerous. It is rare and increases the chance of developing cancer by 5-10%.
- Congenital anomalies of the biliary tract. Anomalies such as choledochal cysts, which some people have from birth, may not manifest themselves for a very long time. But they increase the risk of bile duct cancer by 30%. Hereditary pathological anomaly Caroli syndrome can also lead to the development of malignant neoplasms.
- Parasites. Chronic parasitic diseases such as opisthorchiasis (which can be contracted through fish) are a risk factor for bile duct cancer.
- Some diseases. For example, gallstone disease can cause inflammation and, consequently, cancer. Normal liver tissue with cirrhosis turns into scar tissue, which contributes to the occurrence of tumors. Patients with chronic ulcerative colitis often have sclerosing cholangitis. Chronic hepatitis B and C also increase the likelihood of developing bile duct cancer.
Risk factors also include alcoholism and smoking, overweight and diabetes, non-alcoholic fatty liver disease, chronic pancreatitis, exposure to certain substances such as radon, dioxins, asbestos, etc.
Symptoms of bile duct cancer
Bile duct cancer practically does not manifest itself in the early stages of development. Symptoms appear when the tumor already interferes with the passage and outflow of bile through the ducts. Even later, symptoms appear if it is cancer of the intrahepatic bile ducts.
Universal and most common symptoms include:
- Mechanical jaundice. It manifests itself in dark yellow coloration of the skin, sclera of the eyes, mucous membranes. The reason for the yellow color is the entry of bilirubin into the blood due to the fact that the outflow of bile is impaired.
- Skin itch. He is often out of control. This is also a manifestation of an increased level of bilirubin in the blood.
- Darkening of urine and lightening of feces. This is due to the fact that bile does not enter the intestines, and the body tries to excrete excess bilirubin through the kidneys and urine.
- Pain in the upper abdomen on the right side.
- Lack of appetite or decreased appetite.
- Nausea, maybe vomiting.
- Weight loss.
- Fever.
The clinical picture of bile duct cancer is complemented by the fact that the body is poisoned by bile formation products in the liver, which primarily destroy its cells. Blood clotting is impaired.
But the presence of these symptoms does not mean oncology. Bile duct cancer is rare, and the symptoms described above are more likely to indicate diseases of the gallbladder, liver, or pancreas. But in order to exclude oncology, and in case of cancer, to start its treatment as soon as possible, you need to be examined by a doctor. You can do this in our clinic by calling or signing up for an online consultation.
Stages of bile duct cancer
The most common staging system for bile duct cancer (like any other cancer) is the TNM system. It is named after three indicators: T - the size of the primary tumor, N - the number of affected regional lymph nodes, M - the presence or absence of distant metastases. Each indicator is accompanied by a number indicating the degree of expression of this feature. In the process of development, the tumor in the biliary tract increases in size, can capture neighboring tissues, its metastases affect the nearest lymph nodes, and over time, metastases reach more distant places, where they settle and form new foci.
A more familiar, simplified cancer staging system is as follows:
- Stage 1 - the tumor has not yet spread to neighboring tissues, but is localized only within the bile duct;
- Stage 2 - the lesion begins to invade tissues adjacent to the bile duct (liver, blood vessels, adipose tissue - depends on the location of the tumor)
- Stage 3 - the degree of spread of the tumor to neighboring tissues increases and in parallel the cancer captures the lymph nodes
- Stage 4 - metastases have appeared in other organs - distant parts of the liver, lungs, bones, peritoneum, etc.
There are slightly different staging classifications separately for intrahepatic bile duct cancer and extrahepatic bile duct cancer, which take into account the location of the tumor and adjacent structures, organs, and tissues.