Arthroscopy
Arthroscopy is a method that allows an optical video system to be inserted into the joint through a special "puncture" and to examine it completely. Arthroscopy provides an accurate diagnosis, makes it possible to see damage to the meniscus and ligaments, and identify the true cause of pain. And this is often difficult to establish not only with a conventional, but also with magnetic resonance imaging.

specialists

equipment

treatment






Advantages of joint arthroscopy
Minimal invasiveness of the operation. For example, most often for arthroscopy of the knee joint, anterior internal and anterior external approaches are used on the sides of the patellar ligament with dimensions of 3-5 mm for optics and arthroscopic instruments. These approaches make it possible to examine almost all parts of the joint and eliminate most intra-articular problems. A complete diagnosis of knee joint pathology is approaching 100%.
Arthroscopy of the knee joint helps to examine almost all parts of the joint and assess the functional state of the joint without compromising its anatomical integrity. Joint arthroscopy does not require long-term rehabilitation. After the operation, early weight-bearing on the limb is possible, walking without additional support is possible after 1-3 days, the period of disability is reduced from 4-6 weeks to 2-3 weeks. Such results are especially important for young people and professional athletes, since it becomes possible to start training as soon as possible and compete in competitions in a very short period of time. Reducing hospital stay for arthroscopy of any large joint. Discharge from the hospital after joint arthroscopy occurs within 1-3 days after the operation.
Indications for knee arthroscopy

At Clinic+31, knee arthroscopy is prescribed in the following cases:
- Damage to the menisci. The modern equipment of the orthopedics-traumatology department of Clinic+31 and the qualifications of our specialists allow us to perform not only resection of the damaged meniscus, but, if indicated, also its suture.
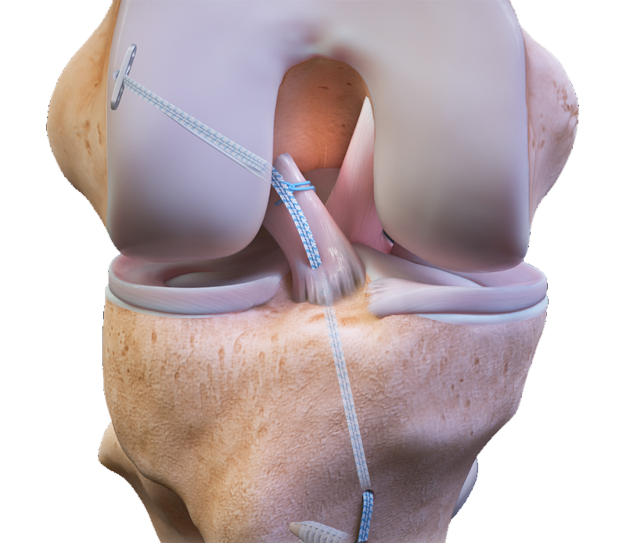
- Injury to the cruciate ligaments of the knee
- Inflammatory diseases of the synovial membrane
- Habitual luxation of the patella
- Inflammatory diseases of the synovial membrane
- Damage and disease of articular cartilage
- Deforming arthrosis of the knee joint
- Rheumatoid arthritis
- Hoff's disease: damage and disease of the fat body - chronic hyperplasia of the fat body
- Unclear pathologies due to damage or disease of the joints, the causes of which have not been identified using clinical and instrumental research methods
- Unclear complaints after previously performed surgical interventions
General information
Types of operations on the shoulder joint
Arthroscopy of the shoulder joint is performed for diagnostic and treatment purposes. Accurate diagnosis is important for young patients and is especially important in cases where other research methods do not allow a definitive diagnosis. Joint arthroscopy provides important information about the nature of damage to the biceps tendon and rotator cuff, and helps to establish the causes of the inability to move the arm in the shoulder joint.
Specialists at the Department of Traumatology and Orthopedics at K+31 perform the following types of operations on the shoulder joint:
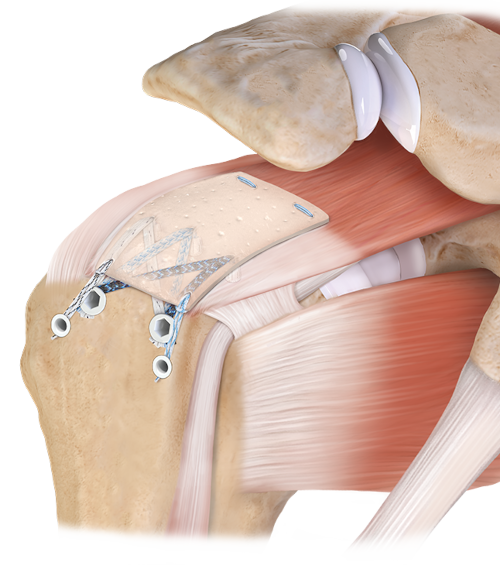
- Rotator seam
- Decompression of the subacromial space with “impingement” syndrome
- Fixation of the cartilaginous lip and capsular-ligamentary complex in case of joint instability.
It is often necessary to perform arthroscopic refixation of the labrum (in case of a Bankart injury or SLAP injury), or tenodesis. In this case, both for stitching and for fixing the torn section of the articular labrum to the edge of the glenoid cavity, special titanium or absorbable arthroscopic anchors are used.
Our doctors










































This award is given to clinics with the highest ratings according to user ratings, a large number of requests from this site, and in the absence of critical violations.

This award is given to clinics with the highest ratings according to user ratings. It means that the place is known, loved, and definitely worth visiting.

The ProDoctors portal collected 500 thousand reviews, compiled a rating of doctors based on them and awarded the best. We are proud that our doctors are among those awarded.
Make an appointment at a convenient time on the nearest date
Price
Reviews

Registration for a consultation




Our clinics

Application “Personal Account K+31”












Advantages of joint arthroscopy